


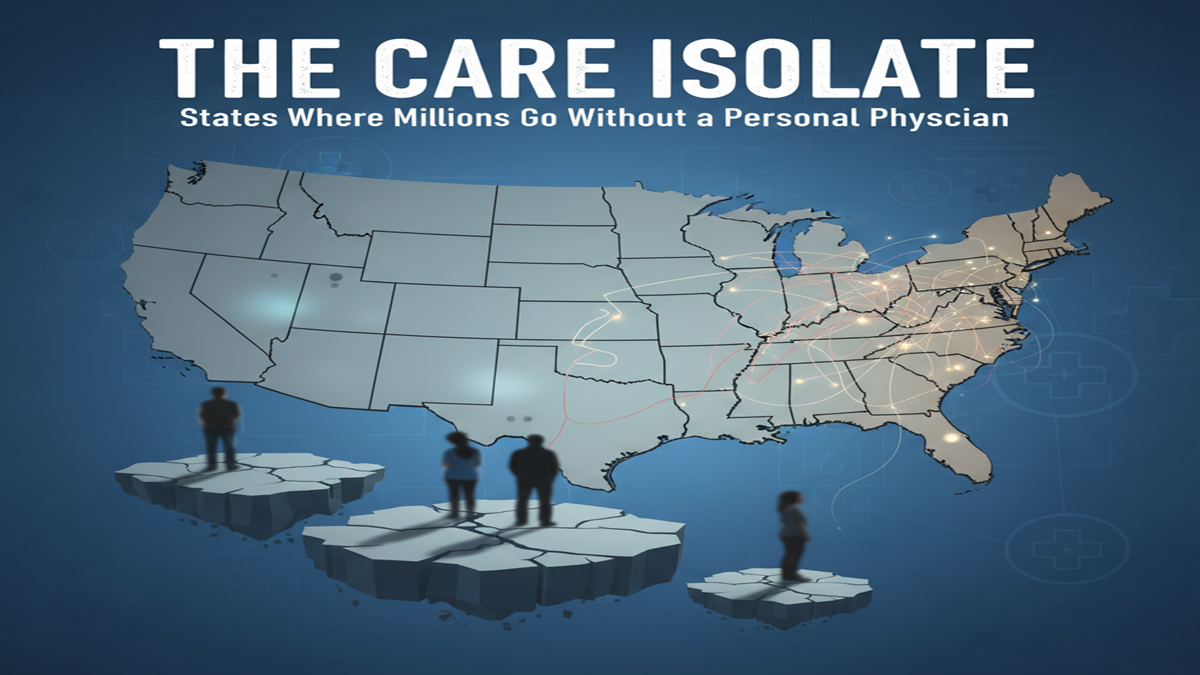
A developing fragment of the American populace is exploring the complex healthcare scene without a individual doctor, a key grapple for steady, preventative care. A state-by-state investigation uncovers tremendous incongruities in get to, highlighting a deep-seated emergency with significant suggestions for open wellbeing results and spiraling costs.
According to later information from organizations like KFF, about one in five U.S. grown-ups detailed not having a individual doctor or healthcare supplier, a national figure that covers serious state-level contrasts. The rankings appear a stark topographical partition, with states like New Mexico and Nevada detailing the most noteworthy rates—around 29% and 26.8%, respectively—while states in the Northeast, such as New Hampshire and Maine, keep up the most reduced, drifting between 9% and 9.2%.
Background and Verifiable Setting: The Roots of the Shortage
The current get to emergency is not an overnight marvel but a summit of decades-long approach choices and statistic shifts.
In the late 20th century, especially taking after the Graduate Medical Education National Advisory Committee (GMENAC) report in 1980, the U.S. executed a medical school moratorium to avoid an expected overflow of doctors. This driven to a solidify and diminishment in therapeutic school enrollment that kept going into the early 2000s, definitely abating the pipeline of unused doctors.
While therapeutic school enrollment has since expanded, the supply of residency slots—funded to a great extent by Medicare—has not kept pace with populace development, making a bottleneck that anticipates numerous restorative school graduates from completing their training.
- 1980s Ban: A approach choice that misleadingly obliged the supply of doctors, the impacts of which are still felt today.
- Primary Care vs. Strength: Truly, essential care doctors (PCPs) get lower remuneration than pros, driving less restorative understudies to select family pharmaceutical, inner pharmaceutical, or pediatrics.
- Rural-Urban Separate: Doctor dissemination has long favored urban and well-off zones, taking off country and underserved communities with persistent deficiencies, regularly alluded to as “therapeutic deserts.” The Health Resources and Administrations Organization (HRSA) as of now assigns thousands of essential care Wellbeing Proficient Deficiency Zones (HPSAs), affecting tens of millions of people.

Current Patterns: An Maturing Populace Meets a Extended Workforce
The challenge is being intensely exacerbated by effective, meeting trends:
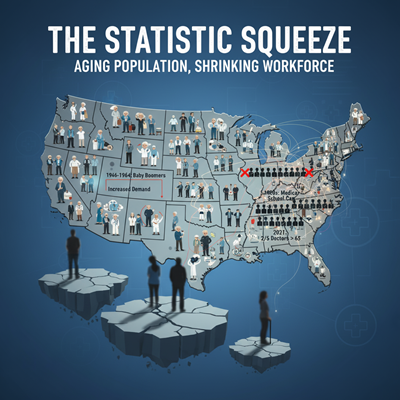
The Statistic Squeeze
The maturing of the U.S. population, driven by the Child Boomer era, is definitely expanding the request for essential care administrations, as more seasoned grown-ups ordinarily have more incessant conditions and complex healthcare needs. At the same time, the physician workforce itself is aging, with over two in five dynamic doctors anticipated to be 65 or more seasoned by 2031, signaling a coming wave of retirements.
The Rise of Non-Traditional Models
In reaction to long hold up times and high-volume hones, modern models are picking up traction:
- Direct Essential Care (DPC) and Concierge Medication: These models charge an yearly enrollment charge, promising patients way better get to and more time with their specialist by constraining the quiet board measure. Whereas giving great care for those who can manage it, specialists note this advance compounds the weight on conventional hones by taking doctors out of the common network.
- Consolidation: The proprietorship of essential care hones is progressively solidifying beneath huge clinic frameworks or private value firms, which can lead to shifts in hone center that prioritize income over accessibility.
Expert Supposition: The Suggestions for Open Health
Public wellbeing specialists and policymakers consistently push the basic part of having a individual doctor, frequently alluded to as having a “therapeutic home.”
Dr. Anna Patel, a wellbeing approach investigator, emphasizes the systemic disappointment: “The need of a individual doctor implies a need of care coordination. It’s not fair almost check-ups; it’s approximately having a single point of contact who gets it your whole restorative history, oversees your constant conditions, and arranges referrals to specialists.”
Research reliably joins vigorous essential care get to to made strides wellbeing results and lower in general healthcare costs:
- Increased Life Hope: Considers have appeared that an increment in the proportion of essential care doctors per populace is related with a quantifiable increment in life expectancy.
- Reduced Crisis Room Utilize: Patients with a steady PCP are essentially less likely to depend on exorbitant crisis office visits for non-urgent issues, lessening strain on the whole system.
- Better Unremitting Infection Administration: Conditions like diabetes and hypertension are overseen more successfully, anticipating exorbitant hospitalizations and complications.
The Real-World Suggestions of the Get to Gap
The abberations in state rankings—with Western, Mountain, and a few Southern states topping the list for need of a PCP—reflect more profound issues of destitution, supplier thickness, and rurality.
The human fetched is measured in deferred analyze and poorer quality of life:
- Delayed or Conceded Care: People without a PCP are more likely to delay fundamental preventive administrations, such as cancer screenings and immunizations, or delay looking for treatment for minor side effects until they ended up serious and require costly, intense intervention.
- Health Value and Incongruities: The need of get to excessively influences uninsured and low-income populaces, as well as minority and rustic communities, extending existing wellbeing incongruities and sustaining cycles of destitute health.
- Fragmented Care: Patients without a devoted specialist regularly cycle through critical care clinics and crisis rooms, driving to divided and verbose care where no single proficient has a comprehensive see of their health.
Addressing this basic get to hole requires a multipronged approach: expanding government financing for residency preparing, especially for essential care and in underserved regions; inventive conveyance models utilizing telehealth and team-based care; and approaches that incentivize specialists to hone in high-need districts. Until at that point, millions of Americans will proceed to look for wellbeing without a trusted direct.

